
Recent Posts
February 2024
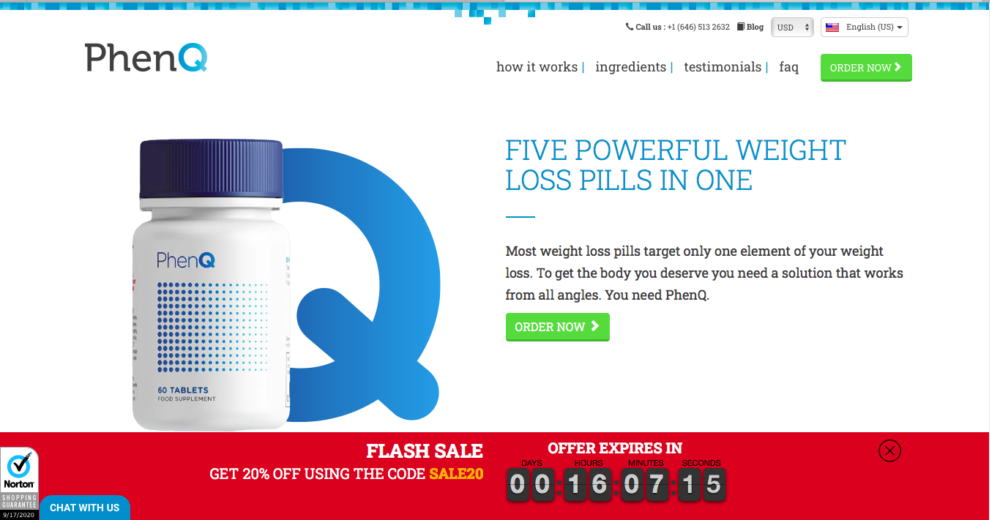
PhenQ Detailed Review (2024) | Is it still the Best Weight loss Pill ?
This Updated Review provides a more comprehensive analysis and a [...]
October 2023

Intermittent Fasting Diet in Bodybuilding
Here is an interesting case. Is there a combination of [...]

Viasil Detailed Review | Is it the Best Male Performance Enhancer?
Erectile dysfunction, or even erectile impotence, two medical terms almost [...]
January 2022


Leanbean | Review 2022 | Fat Burner especially For Women
What would you think when you hear that, there are [...]
December 2021
10 Best Legal Steroids [2022 Updated] | That Work Safe and Fast!
Talking about muscle mass and muscle gains in general, a [...]
Top Articles of 2021
10 Best Legal Steroids [2022 Updated] | That Work Safe and Fast!
Talking about muscle mass and muscle gains in general, a [...]

Best Weight Loss Pills | Review [2021 Updated] | “TOP 10” Right NOW
Today's article intended to bring together Best Weight Loss Pills [...]

Best ED (over the counter) Pills * Erectile Dysfunction *
The modern man, carrying numerous responsibilities and a high level [...]

Best Immune System Booster Supplements | Review 2021
A strong immune system and a powerful and ready to [...]

Best Testosterone Booster Supplements [2021] | Top (5) Results
Today's article is all about Best Testosterone Booster Supplements and [...]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Best Natural Steroids | Go for the effective, safe & affordable way
A large majority of people would classify the anabolic steroid, [...]
About Intarchmed
 Intarchmed (International Archive of Medicine and Supplements) offers a broad range of:
Intarchmed (International Archive of Medicine and Supplements) offers a broad range of:
• honest reviews (based on personal experience of our authors) on all products (BodyBuilding, Weight Loss, Fitness etc.)
• ways to avoid being misled by various crooks wishing to deceive you with ineffective & dangerous preparations
• Effective natural methods to boost your body and make you healthier
• Smart tricks to trick the time passing by and affecting your body
• products assisting physically, mentally, as well as psychologically, uplifting your life
• valuable small secrets and general info on how to get the fastest & most effective muscle gains